Introduction: why TCM for RA?
Rheumatoid arthritis (RA) is a chronic autoimmune disease with synovitis, joint destruction, and systemic inflammation. Despite available disease‑modifying antirheumatic drugs (DMARDs) and biologics, a significant proportion of patients respond insufficiently or experience adverse effects. In China, Traditional Chinese Medicine (TCM) has been used for centuries, and recent decades have yielded extensive clinical and mechanistic evidence. The best‑studied agents are Lei Gong Teng (Tripterygium wilfordii Hook F, TwHF) and the formula Simiao Yong'an Decoction. This review summarizes the evidence.
Clinical evidence: Tripterygium wilfordii (TwHF)
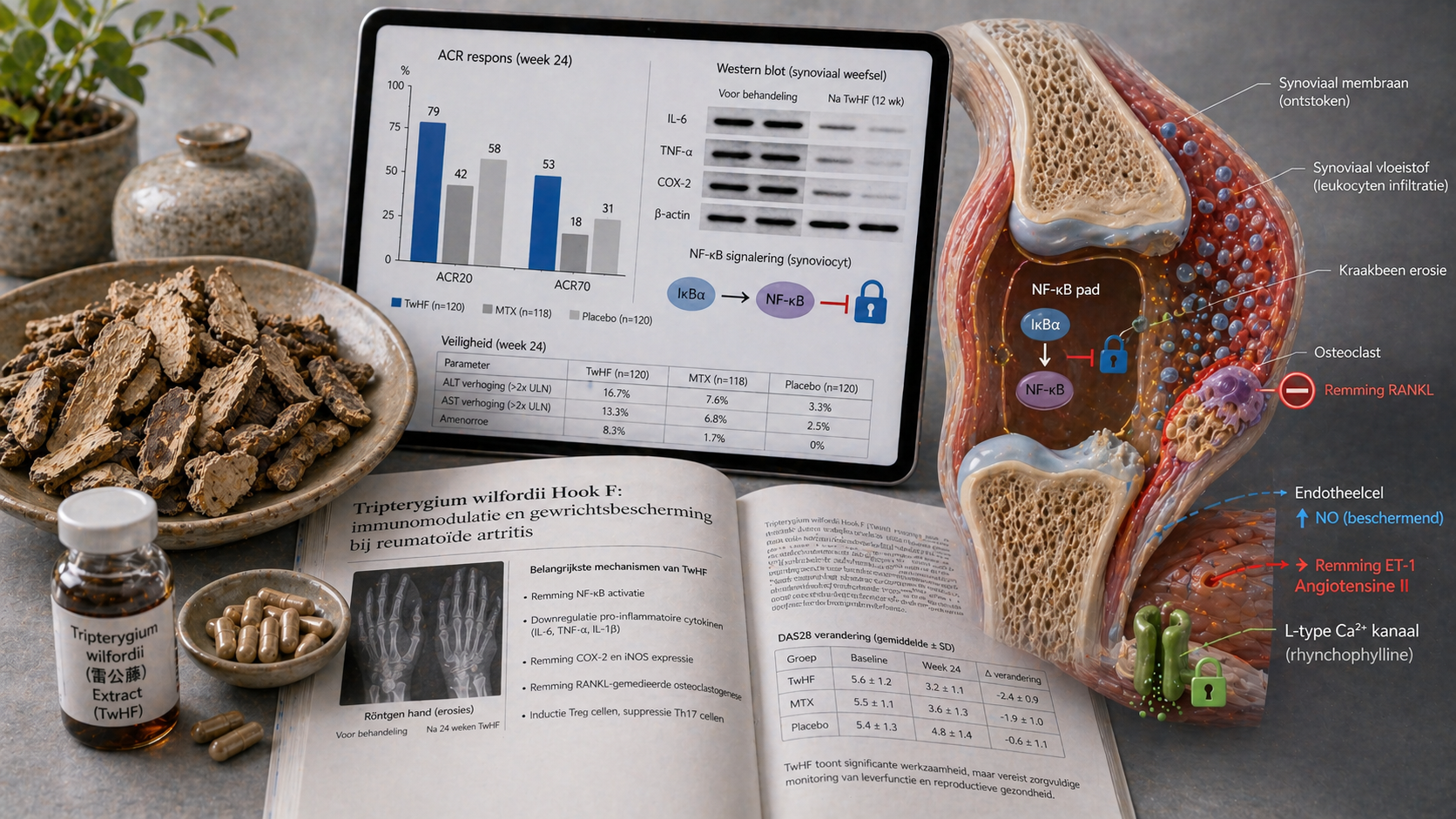
A 2025 meta‑analysis of 15 randomized controlled trials with 1,826 RA patients compared TwHF extract (± conventional DMARDs) with placebo or DMARDs alone. TwHF improved ACR20 response (RR 1.68, 95% CI 1.42‑1.98), significantly reduced swollen and tender joint counts (SMD −1.21, 95% CI −1.58 to −0.84), and lowered the DAS28 disease activity score (mean difference −1.08, 95% CI −1.37 to −0.79). A Chinese multicenter RCT (2024, n=360) showed that a standardized TwHF extract (triptolide 1 mg/day) plus methotrexate (MTX) was superior to MTX alone after 24 weeks: ACR70 response 34% vs 18% (p<0.01).
Other formulas: Simiao Yong'an Decoction and Qingluo Yin
Simiao Yong'an Decoction (Simiao Yong'an Tang) is used in China for ''heat‑toxin'' arthritis. An RCT (2025, n=240) of this formula plus MTX vs MTX alone showed greater reduction in anti‑CCP antibodies and MMP‑3, and slowed radiographic progression (modified Sharp score). Qingluo Yin (a formula of Scutellaria, Coptis, Phellodendron) reduced morning stiffness and IL‑6 levels in an open study (n=160).
Mechanisms: immunomodulation and anti‑inflammation
Preclinical and clinical studies have elucidated the main mechanisms:
• **T‑cell regulation**: TwHF suppresses CD4+ T‑cell activation and reduces IL‑17 and TNF‑α production.
• **NF‑κB inhibition**: Triptolide (the active component) blocks the NF‑κB signaling pathway, reduces pro‑inflammatory cytokines (IL‑1β, IL‑6, TNF‑α), and downregulates COX‑2 and iNOS.
• **Synovial fibroblasts**: TwHF induces apoptosis of fibroblast‑like synoviocytes (FLS) via the mitochondrial pathway and inhibits invasion and matrix metalloproteinase (MMP) release.
• **B‑cell response**: Tripterygium lowers anti‑CCP and rheumatoid factor titers and plasma cell differentiation.
• **Osteoclastogenesis**: TwHF inhibits RANKL‑mediated osteoclast differentiation, thereby reducing bone erosion.
Safety aspects of Tripterygium
TwHF is effective but has a narrow therapeutic window. Adverse effects include gastrointestinal (diarrhea, nausea), amenorrhea (due to gonadotoxicity), skin rash, and mild liver enzyme elevation. In the RCTs, the drug was stopped when significant liver abnormalities (ALT >3x ULN) occurred or in women planning pregnancy. Cardiovascular adverse events (hypotension) have been reported at high doses. In China, TwHF is used only in patients with active, treatment‑resistant RA under strict monitoring. Standardized extracts with lower triptolide content are being developed to improve safety.
Position in Chinese guidelines
The Chinese Guideline for the Diagnosis and Treatment of Rheumatoid Arthritis (2024) advises TwHF (standardized extract) as add‑on therapy after insufficient response to MTX or leflunomide (class IIa, level B). The guideline emphasizes that TwHF must not be used during pregnancy, in children, in renal insufficiency, or in severe liver disease. Simiao Yong'an Decoction is recommended for the pattern ''heat‑toxin obstructing the meridians''.
Conclusion for clinical practice
For Western clinicians: consider adding a standardized Tripterygium extract (under strict monitoring of liver, renal function, and CBC) for an RA patient with insufficient response to MTX (DAS28 >3.2) and no pregnancy wish. Consult a TCM practitioner for pattern diagnosis (heat‑toxin, cold‑damp, qi‑blood stasis). Current evidence – including meta‑analyses and RCTs – supports an integrated approach, provided the patient is well informed about the risks of TwHF.